You have probably heard about it; you may even probably be suffering from it. Melasma is a very common pigment problem in Singapore, however, treatments that give effective results are unfortunately, not as common.
Can melasma really be treated permanently? What then are the treatments that really work, how should these treatments be done, and what are the things you can do on your own to aid in improving your melasma? Read on to find out more.
What Is Melasma?
Melasma is a chronic pigmentation condition that shows up as brown or grey-brown patches, usually on the cheeks, forehead, nose, upper lip and jawline. It’s especially common in female patients, starts showing up around the childbearing years and is driven by a mix of genetics, hormones, and environmental stimulation, not just “too much sun.”

Unlike a sunspot or an acne mark, melasma:
- Develops gradually, often deep in the skin’s pigment-producing layer
- Can keep progressing even with consistent skincare
- Frequently returns after successful treatment if triggers aren’t managed
- Affects visible, hard-to-hide areas of the face (eg. on the cheek prominences and nose bridge), which is why many patients describe a real emotional toll, not just a cosmetic one
Why Is Melasma So Common in Singapore?
Singapore’s climate and population make it something of a perfect storm for melasma:
| Factor | Why It Matters |
|---|---|
| Year-round UV exposure | Constant melanocyte stimulation, no “off season” for the skin |
| High visible-light, blue light and other sources of indoor light exposure | Light from personal devices, sunlight reflecting off windows, can worsen pigment with chronic exposure, even with sunscreen on |
| Fitzpatrick skin types III-V common in Asian skin types | These skin types are naturally more reactive to pigment-triggering stimuli |
| Heat and humidity | Heat alone can also activate pigment-producing cells, independent of UV |
Even people who stay indoors most of the day aren’t fully protected – visible light exposure through windows and daily outdoor transit time is enough to keep triggering pigment in susceptible skin.
What Causes Melasma?
1. Sun and Visible Light

UV radiation stimulates melanocytes (the skin’s pigment-producing cells) into overdrive. But UV isn’t the whole story – heat and visible light also play a role, which is why some patients keep flaring even with regular sunscreen use. Think of melanocytes as an alarm system that gets more sensitive each time it’s triggered; over time, even small exposures set it off.
2. Hormones

Pregnancy, oral contraceptives and hormone replacement therapy are all associated with melasma onset or worsening. This is well documented and is one reason melasma is sometimes called the “mask of pregnancy.”
3. Genetics
A family history of melasma meaningfully raises your own risk. This is one of the more under-discussed drivers and it’s why some patients develop melasma with minimal sun exposure while others with heavy sun exposure never do.
4. Inflammation

Anything that irritates the skin (over-exfoliation, aggressive facials, harsh peels) can also trigger or worsen pigment in melasma-prone skin. This is a key reason treatment choice matters so much more.
Why Melasma Is Hard to Treat
@ishiniw Brown skin WOC have been lied to long enough 😩 no more spending hundreds or even thousands of dollars on one product fixes all BS… I hate to break it to you but there are systems and lifestyles shifts that need to be made to see a difference and that by first being able to differentiate the two ✨ #hyperpigmentation #melasma #pcos #irondeficiency #brownskin
Melasma behaves like a chronic condition to be managed, not a stain to be removed once. A helpful way to think about it: it’s less like a paint stain and more like a weed with deep roots. Clearing the visible pigment doesn’t remove the underlying tendency for your body to make more of it.
Realistic expectations matter. Success is measured by:
- Visible reduction in pigment intensity
- Longer intervals between flare-ups
- Better control with less aggressive intervention over time
Recurrence after initially successful treatment is extremely common, especially when sun protection or maintenance skincare lapses. This is one of the most consistent findings in melasma literature and clinical experience alike.
Melasma Treatment Options in Singapore
Topical (Prescription Cream) Treatments
| Ingredient | How It Works | What to Know |
|---|---|---|
| Hydroquinone | Reduces melanin production | Effective but needs medical supervision. Prolonged unsupervised use carries a small risk of a blue-grey skin discolouration called exogenous ochronosis, so it’s typically prescribed in cycles. |
| Triple combination cream (hydroquinone + retinoid + mild steroid) | Targets pigment from multiple angles | Often faster-acting than hydroquinone alone. Medical supervision required as well. |
| Tranexamic acid (topical or oral) | Reduces the vascular/inflammatory signalling that feeds melasma | Increasingly popular for stubborn or recurrent cases; oral use requires screening and a doctor’s assessment |
| Cysteamine cream | Blocks pigment production through a different pathway to hydroquinone | A useful non-hydroquinone option, especially for patients who can’t tolerate hydroquinone or need a break from it; the main downside is a sulphur-like smell during application, and mild irritation in some patients |
| Antioxidant skincare regime (vitamin C, niacinamide, and similar) | Calms inflammation and limits new pigment triggers day to day | Not a primary treatment on its own, but a genuinely important foundation.This is the daily regime that protects results from any of the treatments above and reduces flare-ups between them |
Procedural Treatments
Chemical peels Superficial-to-moderate peels can help lift surface pigment and improve how well topical treatments penetrate. In Asian skin, gentler protocols are safer, while aggressive peels can provoke more pigmentation rather than fix it, so my advice is to proceed with caution.
Medical laser treatment “Laser for melasma” isn’t a single treatment. Several different laser types can help, and they don’t all work the same way:
- Q-switched lasers is a longer-established option, very effective at breaking down pigment
- Pico lasers has recently been popular, containing ultra-short pulses that break up pigment with minimal heat
- Vascular lasers target the underlying blood vessel component that often feeds stubborn melasma
- CO2 lasers used more selectively, typically for resistant cases needing deeper resurfacing

No single laser addresses every driver of melasma. This is why combination laser treatment, that is, using two or more of these types together, tailored to the individual case, is generally preferred. This method is more effective than relying on one laser type (such as Pico alone). Each laser interrupts a different part of how melasma forms, so combining them addresses more of the problem at once.
A word of caution on lasers generally: NOT every laser is appropriate for melasma and the WRONG device or settings can worsen it. This is the single biggest reason to have melasma properly assessed. The severity of the melasma, the location of the pigmentation within the skin (epidermal, dermal or mixed), its main biochemical cause, all has an implication on its prognosis, and thus its treatment plan.
Quick Comparison
| Treatment | Effectiveness | Recurrence Risk | Best For |
|---|---|---|---|
| Hydroquinone / triple cream | High | Moderate (if stopped abruptly) | Epidermal (surface-level) melasma |
| Tranexamic acid | High | Moderate | Hormonal or vascular-driven melasma |
| Cysteamine cream | Moderate-High | Moderate | Patients unsuitable for or rotating off hydroquinone |
| Chemical peels | Moderate | Moderate | Superficial pigmentation, as an adjunct |
| Medical laser (single type, e.g. Pico alone) | Moderate-High | High without maintenance | Resistant cases, as part of a broader plan |
| Combination laser treatment (e.g. Pico + Q-switched or vascular) | High | Moderate with maintenance | Resistant or mixed-depth cases needing a multi-pathway approach |
| Antioxidant skincare regime (vitamin C, niacinamide) | Supportive, not standalone | N/A – reduces recurrence of other treatments | All patients, as a daily foundation |
| Tinted sunscreen (SPF 50+, iron oxide) | Essential | Reduces recurrence significantly | All patients |
What Actually Works: The Evidence
The consistent theme across dermatology guidance is that melasma responds best to combination therapy, not any single product or procedure. A typical evidence-based framework:
- Prescription topical treatment (hydroquinone, triple cream, tranexamic acid, or cysteamine cream)
- A consistent antioxidant skincare regime (vitamin C, niacinamide) to support and protect results
- Daily broad-spectrum, visible-light-blocking sunscreen, with good SPF and PA ratings
- Trigger avoidance (heat, harsh actives, hormonal contributors where modifiable)
- Procedural treatment only where topicals plateau. Ideally combination laser therapy rather than a single laser type, and only with a conservative, Asian-skin-appropriate protocol
Sunscreen: Why checking SPF Value Alone May Not Be Enough

Standard sunscreens are formulated to block UVB, BUT visible light is a separate trigger that plain SPF doesn’t fully address. In addition, besides UVB that is responsible for sunburns, we need to be concerned about UVA as well, as these ultraviolet rays accelerate skin aging, wrinkles and loss of collagen in the patients.
Furthermore, the SPF value is only applicable within a short time frame. Without reapplying sunscreen, within 1 hour of sunscreen application, the SPF protection value of the sunscreen will have degraded significantly. This is why many patients apply sunscreen faithfully and still see flare-ups or pigmentation progression.
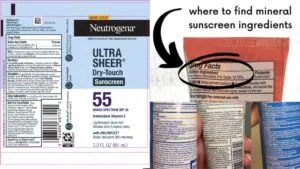
What to look for:
- SPF 50+, broad-spectrum
- PA +++ or higher to screen out UVA
- Physical filters containing zinc oxides or titanium dioxide
- Chemical filters that are photostable and non-irritating to the skin
- Tinted sunscreens, or sunscreens with some iron oxides within are preferred
- Reapplied through the day, not just applied once in the morning
- Paired with physical sun avoidance (hats, shade, timing outdoor activities)
Choosing a Clinic: Questions Worth Asking

Before starting treatment, it’s worth asking your practitioner:
- What type of melasma do I have, for instance epidermal, dermal, or mixed?
- What combination of treatments your doctor will recommend, and why?
- How many sessions or how many months before you expect to see change?
- What’s my maintenance plan once pigment improves?
- What’s my realistic recurrence risk, and how do we manage it?
- If a laser is recommended, is it a single laser type or a combination approach, and why?
- Are there any non-laser alternatives worth trying first?
Clinics offering an individualised assessment, rather than a fixed “melasma package”, tend to set more personalised treatment goals and therefore deliver better long-term outcomes.
The Bottom Line
There’s NO single product or one-time procedure that permanently erases melasma.
It’s a chronic, multifactorial condition that is driven by lifestyle, hormones, genetics, and underlying skin inflammation. We believe that melasma responds best to a combined and consistent approach the right prescription topical, effective sun protection, and procedural treatment used judiciously, at the right time and duration.
The goal isn’t perfection. It’s durable control of the melasma severity and an overall healthier skin.
FAQs
Can melasma be cured permanently? No. Melasma is a chronic condition. It can be significantly improved and controlled, but it can return if underlying triggers, like sun exposure, hormones, heat, inflammation, become active again.
Is laser treatment the best option for melasma? Usually not on its own. Lasers can help selected patients, but the wrong laser or settings can worsen melasma. Several laser types exist, for instance Pico, Q-switched, vascular, CO2. Combining more than one type is often more effective than relying on a single laser, since each addresses a different part of the melasma development.
How long does it take to see results? Many patients can notice improvement within 6 to 12 weeks of consistent, disciplined treatment, though full management is typically measured in months, not weeks.
What sunscreen is best for melasma? A mineral, SPF 50+, PA +++ sunscreen containing titanium dioxide or zinc oxide or chemical filters, or a combination of the above. This protects against both UVA and UVB.
Does melasma get worse with age? It can become more persistent if triggers stay active over time, but consistent treatment and daily sun protection help prevent progression.